Leaky Gut and Menopause: Is Intestinal Permeability Behind Your Symptoms?
The term “leaky gut” has a credibility problem. It sounds like wellness marketing. It gets dismissed in some clinical circles as an imprecise, overused concept. And it has been co-opted by supplement companies selling expensive products to anxious women who are told their gut is the root of everything wrong with them.
So let me be clear about what this article is and is not.
It is not a case for leaky gut as a cure-all explanation or a justification for any particular supplement protocol. It is a clear-eyed look at the peer-reviewed evidence on intestinal permeability — what it is, how it develops, how it interacts specifically with the hormonal changes of perimenopause, and what the research shows about addressing it through food.
Because the evidence is genuinely significant. Intestinal permeability is not a fringe concept — it is a measurable physiological state with well-established mechanisms that connect directly to the cluster of symptoms most perimenopausal women are dealing with: systemic inflammation, joint pain, brain fog, bloating, fatigue, and mood instability.
Understanding it properly — stripped of the hype — is one of the most useful things you can do for your symptom management.
Episode: “Leaky Gut and Menopause — The Evidence Without the Hype” — Real Food Science Podcast
Key Takeaways
- Intestinal permeability is a real, measurable physiological state — not a wellness myth
- Oestrogen directly maintains the tight junction proteins that hold the gut lining together; as oestrogen declines in perimenopause, gut permeability increases
- Increased permeability allows bacterial fragments called lipopolysaccharides (LPS) to enter the bloodstream, triggering the systemic inflammatory cascade behind many menopause symptoms
- The foods driving gut permeability — seed oils, emulsifiers, alcohol, ultra-processed foods — are the same foods driving broader inflammation in perimenopause
- Gut permeability is highly responsive to dietary change — measurable improvements in tight junction integrity have been observed within two to four weeks of sustained dietary intervention
- The 7-Day Anti-Inflammatory Food Swap Guide is the fastest practical entry point for reducing the dietary inputs that maintain gut permeability
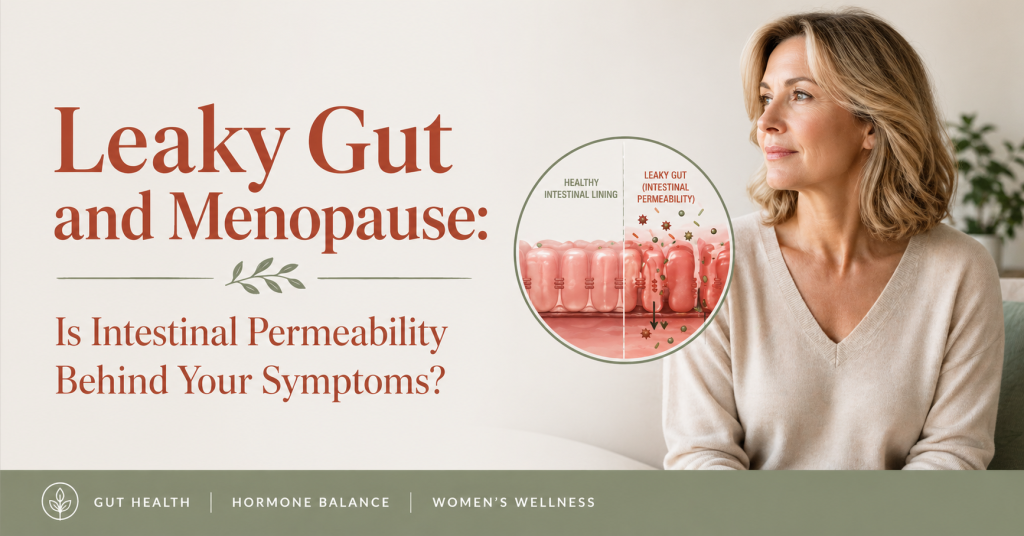
What Intestinal Permeability Actually Is
Your gut lining is a remarkable structure. It is a single cell layer thick — one cell. These epithelial cells line the approximately eight metres of your small and large intestine, forming the barrier between the contents of your gut — food particles, digestive enzymes, bacteria, bacterial metabolites — and your bloodstream.
This barrier is meant to be selectively permeable. Its job is to absorb nutrients — amino acids, fatty acids, glucose, vitamins, minerals — while keeping everything else out. The cells that do this job are held together by a network of proteins called tight junctions: specifically claudin, occludin, and zonulin. When these proteins are functioning correctly, the gaps between epithelial cells are effectively sealed.
Intestinal permeability — the clinical term for what is colloquially called leaky gut — is the state in which these tight junction proteins become dysregulated, loosening the seals between cells and allowing molecules to pass through that should not. This is not a metaphorical “leakiness” — it is a measurable increase in the paracellular transport of molecules across the gut wall, quantifiable through lactulose/mannitol ratio testing, serum zonulin measurement, and other validated clinical assays.
What passes through when permeability increases matters enormously. The most clinically significant are lipopolysaccharides (LPS) — fragments of the outer membrane of gram-negative bacteria that colonise the gut in enormous quantities. LPS molecules are strongly immunogenic — your immune system is exquisitely sensitive to them because they are a reliable signal of bacterial invasion. When they appear in the bloodstream in significant quantities, the immune response is rapid, systemic, and inflammatory.
This is not a theoretical process. A 2007 landmark paper by Patrice Cani and colleagues in Diabetes demonstrated that feeding mice a high-fat, low-fibre diet produced a two to three times increase in serum LPS within weeks — a state they termed “metabolic endotoxaemia.” Subsequent human research confirmed that metabolic endotoxaemia occurs in response to high-fat ultra-processed meals in human subjects, producing a post-meal inflammatory spike that correlates with LPS passage across a compromised gut barrier.
Why Perimenopause Specifically Increases Gut Permeability
Gut permeability has many drivers — diet, stress, medications, ageing. But perimenopause introduces a specific and often underappreciated contributor: the decline of oestrogen.
Oestrogen receptors are expressed throughout the gastrointestinal tract — in the epithelial cells themselves, in the immune cells of the gut wall, and in the enteric nervous system. Oestrogen plays several direct roles in maintaining gut barrier function:

Tight junction protein expression. Oestrogen upregulates the expression of claudin-1, claudin-3, and occludin — the primary structural proteins of tight junctions. Studies using oestrogen receptor knockout models show significantly reduced tight junction protein expression and increased gut permeability compared to controls. As oestrogen declines in perimenopause, this upregulation weakens. A 2020 study in Scientific Reports found that postmenopausal women showed measurably higher intestinal permeability than premenopausal women of comparable age and diet, with the difference correlating with oestrogen levels.
Gut immune modulation. The gut wall houses the largest concentration of immune cells in the body — approximately 70% of the entire immune system. Oestrogen modulates the activity of these cells, particularly mast cells and T-helper cells, reducing their inflammatory tone. As oestrogen falls, gut immune reactivity increases. This is why food sensitivities that were not present in your thirties can emerge in perimenopause — your gut immune system has become more reactive, not because the food has changed, but because the immune modulation that previously prevented reactivity has diminished.
Gut microbiome maintenance. As covered in the gut-hormone connection article, oestrogen supports the growth of Lactobacillus species that produce lactic acid, maintain gut pH, and reinforce the mucus layer overlying the epithelium. The mucus layer is the first line of defence against bacterial contact with epithelial cells — when it thins, bacterial LPS has more direct access to the gut wall.
Gut motility. Oestrogen influences gut transit time through its effects on smooth muscle and the enteric nervous system. As it declines, motility often becomes erratic — alternating constipation and looser stools — which affects the bacterial composition of different gut segments and indirectly increases the load of gram-negative bacteria in the small intestine.
The result of all four mechanisms operating simultaneously is a gut that is structurally more permeable, immunologically more reactive, microbially more disrupted, and functionally less predictable — independent of anything you eat. Diet then acts as an amplifier of this already-compromised baseline.
The LPS-Inflammation-Symptom Chain
Understanding the specific pathway from gut permeability to menopause symptom severity helps explain why a gut-focused approach to menopause nutrition is not peripheral — it is central.
When LPS crosses the gut barrier into the bloodstream, it binds to a receptor called Toll-like receptor 4 (TLR4) on macrophages and dendritic cells throughout the body. TLR4 activation triggers the NF-κB signalling pathway — one of the master switches of inflammatory gene expression. The result is the production of a cascade of pro-inflammatory cytokines: IL-1β, IL-6, IL-8, and TNF-alpha.
These cytokines do not stay local. They circulate systemically and act on multiple target tissues simultaneously:
The hypothalamus. IL-1β and TNF-alpha act on the hypothalamic neurons that regulate the thermoneutral zone — the temperature range within which your body does not trigger a hot flash. Elevated cytokines narrow this zone. This is why systemic inflammation directly increases hot flash frequency and severity — it is not just a correlation, it is a mechanistic pathway from gut permeability to vasomotor symptoms.
Joint tissue. IL-6 and TNF-alpha are the primary cytokines driving inflammatory arthritis and joint inflammation. For perimenopausal women experiencing joint pain and stiffness — a symptom that is frequently attributed entirely to oestrogen decline and frequently undertreated — the LPS-driven cytokine cascade is a significant and addressable contributor.
Brain tissue. LPS crosses the blood-brain barrier and activates microglial TLR4 — the brain’s equivalent of the systemic immune activation described above. Microglial activation produces neuroinflammation that directly impairs synaptic transmission, reduces processing speed, and produces the cognitive symptoms of brain fog. As covered in the brain fog article, neuroinflammation is one of the primary food-modifiable drivers of perimenopause cognitive symptoms.
Adipose tissue. IL-6 and TNF-alpha promote inflammatory activation of adipose tissue — particularly visceral (abdominal) fat. This creates a secondary inflammatory loop: gut permeability drives cytokine production, cytokines activate visceral fat inflammation, activated visceral fat produces more IL-6 and TNF-alpha, which further sensitises the gut immune response. This cycle is one of the mechanisms behind the abdominal weight gain of perimenopause that resists conventional dietary intervention.
Mood and neurotransmitter systems. The cytokine cascade triggered by LPS directly suppresses serotonin synthesis by diverting tryptophan — the serotonin precursor — toward inflammatory kynurenine pathway metabolites. This is the neurobiological mechanism behind the well-established link between systemic inflammation and depression. For perimenopausal women experiencing mood instability, anxiety, or low mood, gut permeability and the associated LPS load is a genuine and often overlooked contributor.
The Dietary Drivers of Increased Permeability
Several dietary factors directly compromise tight junction integrity — either by reducing tight junction protein expression, disrupting the mucus layer, or altering the gut microbiome in ways that increase gram-negative bacterial load.
Seed oils and oxidised lipids. As detailed in the seed oils article and the cooking fats article, high omega-6 polyunsaturated fats and their oxidation products — particularly 4-hydroxynonenal — directly disrupt tight junction protein expression and increase LPS production by the gut microbiome. This is the gut permeability mechanism of seed oil consumption, operating independently of the systemic omega-6/omega-3 ratio effects.
Emulsifiers. Polysorbate-80 and carboxymethylcellulose — two of the most common food emulsifiers, found in ice cream, salad dressings, plant-based milks, processed sauces, and many “health” products — have been shown in controlled studies to directly degrade the gut mucus layer and disrupt tight junction proteins. A 2015 study by Chassaing and colleagues in Nature found that both emulsifiers produced increased gut permeability, altered microbiome composition, and low-grade intestinal inflammation in mice — effects that were subsequently supported in human observational data.
Alcohol. Ethanol is directly toxic to tight junction proteins. Acetaldehyde — the first metabolite of ethanol breakdown — disrupts occludin and claudin expression. Even moderate, regular alcohol consumption produces measurable increases in gut permeability and circulating LPS. For perimenopausal women already dealing with hormonally-driven permeability increases, regular alcohol consumption adds a direct chemical disruption on top.
Refined carbohydrates and added sugar. High glucose availability preferentially feeds gram-negative bacteria — increasing the total gut LPS burden — while simultaneously reducing the prebiotic substrate available for beneficial Lactobacillus and Bifidobacterium species that support the mucus layer. High-glycaemic dietary patterns are consistently associated with higher circulating LPS and greater gut permeability in human observational studies.
Chronic psychological stress. The gut-brain axis operates bidirectionally — and psychological stress directly increases gut permeability through corticotropin-releasing hormone (CRH) and mast cell activation in the gut wall. For perimenopausal women dealing with the compounded stressors of midlife alongside a sensitised HPA axis, stress is a meaningful non-dietary contributor to gut permeability that cannot be addressed through food alone.
The Dietary Healers — What Repairs the Gut Lining
The gut lining has a remarkable capacity for repair — and the evidence for food-based interventions is substantive. Meaningful improvements in tight junction integrity have been observed within two to four weeks of sustained dietary change in multiple clinical studies.
Diverse plant fibre. The single most important gut permeability intervention through diet is increasing the diversity and quantity of plant fibre. Butyrate — produced by gut bacteria fermenting soluble fibre — is the primary energy source for colonocytes, the cells that make up the gut lining. Without adequate butyrate, colonocyte turnover slows and tight junction maintenance is compromised. The resistant starch in cooked and cooled legumes, potatoes, and wholegrains is the most potent butyrate precursor available through food.
Bone broth and collagen-rich foods. Glycine and glutamine — amino acids found in high concentrations in bone broth — are direct fuel sources for enterocytes and are required for tight junction protein synthesis. Several studies have shown that glutamine supplementation reduces gut permeability in clinical populations; bone broth provides both glutamine and glycine in food form. This is one of the most evidence-supported traditional foods for gut healing.
Fermented foods. Kefir, sauerkraut, kimchi, miso, and tempeh introduce live bacterial cultures that compete with gram-negative LPS-producing bacteria, produce short-chain fatty acids that support colonocyte health, and directly support mucus layer production. A 2021 study in Cell by Wastyk and colleagues found that a high-fermented-food diet reduced markers of systemic inflammation including the cytokines associated with LPS signalling.
Polyphenol-rich foods. Quercetin — found in onions, capers, berries, and apples — has been specifically shown in multiple studies to upregulate tight junction protein expression, including claudin-1 and occludin. Berries, green tea, and dark chocolate provide additional polyphenols that support gut barrier function through multiple pathways including antioxidant protection of epithelial cells and anti-inflammatory modulation of gut immune activity.
Extra virgin olive oil. Oleocanthal and other polyphenols in high-quality EVOO have been shown to reduce LPS-induced inflammatory signalling and support the gut microbiome species associated with mucus layer maintenance. Replacing seed oils with EVOO as the primary cooking fat reduces both the direct tight junction disruption of oxidised omega-6 and the LPS production driven by seed oil-altered microbiome composition.
Zinc. Zinc deficiency — common in perimenopausal women due to both dietary insufficiency and stress-driven depletion — directly compromises tight junction integrity. Zinc is required for claudin-1 expression and for the repair of epithelial cell damage. Foods highest in zinc: oysters (the richest dietary source by a significant margin), red meat, pumpkin seeds, legumes, and wholegrains.
What the “Leaky Gut Protocol” Industry Gets Wrong
It would be incomplete to discuss intestinal permeability without acknowledging the supplement industry that has built around it — and what it consistently gets wrong.
The narrative typically goes: you have leaky gut, caused by everything modern, and you need to take L-glutamine, colostrum, deglycyrrhizinated liquorice, zinc carnosine, and a range of other supplements at significant expense to fix it.
The problems with this framing:
First, supplemental L-glutamine has genuinely good evidence in clinical populations with significant gut damage — post-chemotherapy, post-surgery, inflammatory bowel disease. The evidence for supplemental glutamine in the general perimenopausal population is considerably thinner than the marketing suggests. Dietary glutamine from bone broth and protein foods provides meaningful amounts without the supplement cost.
Second, the most important gut permeability interventions — removing seed oils, removing emulsifiers, reducing alcohol, increasing diverse plant fibre and fermented foods — cost less than any supplement protocol and have substantially stronger evidence. No supplement compensates for a diet that continues to directly disrupt tight junctions three times a day.
Third, “leaky gut” is sometimes used to attribute every health complaint to a single cause requiring a single solution. Gut permeability is one contributor to perimenopause symptom burden — a significant one, but not the only one. Food-first approaches work best when combined with the sleep, stress, and hormonal management considerations covered in other articles in this series.
The evidence supports a food-first approach to gut permeability. Supplements can be a useful adjunct in specific circumstances, but they are not the starting point, and they should not be the primary expense.
The 7-Day Swap Approach — Starting Practically
The fastest route into gut permeability repair is not a comprehensive protocol — it is the removal of the most significant daily disruptors and their replacement with gut-supporting alternatives.
This is precisely the framework of the 7-Day Anti-Inflammatory Food Swap Guide linked below: seven daily swaps, each targeting a distinct gut-disruptive input, each with a gut-supportive replacement and the mechanism explained in plain English. By the end of seven days of consistent swapping, the primary dietary drivers of gut permeability — seed oils, emulsifiers, refined carbohydrates, alcohol — are meaningfully reduced, and their replacement foods are actively supporting tight junction repair.
Seven days is not enough to complete gut healing — that takes weeks to months of sustained dietary change. But it is enough to begin it, and for most women it is enough to produce noticeable symptomatic improvements that motivate the continued approach.
Free Resource: Identify Your Bloat Pattern First
Before making wholesale dietary changes, understanding your specific symptom pattern helps you prioritise the interventions most relevant to your gut. The bloating pattern associated with gut permeability — systemic, low-grade, often accompanied by fatigue and brain fog — is distinct from the fermentation-driven bloating of high-FODMAP foods or the motility-related bloating of hormonal changes.
→ Download the free Bloat Trigger Discovery Worksheet — a structured seven-day tracking tool that identifies your personal bloating and symptom pattern so you can target the changes most likely to help you specifically.
Go Deeper: 7-Day Anti-Inflammatory Food Swap Guide
The 7-Day Anti-Inflammatory Food Swap Guide gives you seven direct, practical food swaps — one per day — each with the gut health mechanism explained clearly and the replacement options laid out for every eating occasion. It is the most focused, accessible entry point into addressing gut permeability through food, starting today.
FAQ
Is “leaky gut” a real medical diagnosis? Intestinal permeability is a real, measurable physiological state with validated diagnostic tests. “Leaky gut syndrome” as a clinical diagnosis is not currently recognised by most mainstream gastroenterology bodies — not because the phenomenon is disputed, but because the diagnostic criteria for when increased permeability constitutes a pathological syndrome requiring treatment are not yet standardised. The underlying science of intestinal permeability, tight junction proteins, and their relationship to systemic inflammation is well established in the peer-reviewed literature. The syndrome label is contested; the mechanism is not.
How do I know if I have increased gut permeability? Short of clinical testing — lactulose/mannitol ratio urine test, serum zonulin, or serum LPS — you cannot definitively confirm intestinal permeability at home. However, the cluster of symptoms that correlates with it is fairly characteristic: systemic inflammation that feels disproportionate to obvious causes, food sensitivities that have developed or worsened in perimenopause, bloating that is accompanied by systemic symptoms like fatigue and brain fog, and joint pain that fluctuates with dietary changes. If this cluster describes your experience, the dietary interventions for gut permeability are low-risk and high-benefit regardless of formal confirmation.
Will fixing gut permeability cure my menopause symptoms? Reducing gut permeability addresses one significant contributor to the inflammatory burden that amplifies menopause symptoms — it does not address the hormonal changes themselves. Women pursuing a food-first gut health approach typically experience meaningful reductions in symptom severity and frequency rather than complete resolution. The approach works best as part of a comprehensive strategy alongside adequate sleep, stress management, and medical care where appropriate.
How long does it take to repair intestinal permeability? The gut epithelium turns over approximately every four to five days — one of the fastest cell renewal rates in the body. This means structural repair can begin quickly. Tight junction protein expression can measurably improve within two weeks of removing the primary disruptors and adding gut-supportive foods. Complete restoration of microbiome diversity and mucus layer thickness typically takes four to eight weeks of sustained dietary change. The timeline is relatively fast compared to many dietary interventions — which is one of the reasons gut-focused approaches produce symptomatic improvements that feel disproportionately significant relative to the changes made.
Are probiotics helpful for gut permeability? Certain probiotic strains — particularly Lactobacillus rhamnosus GG, Lactobacillus plantarum, and Bifidobacterium longum — have specific evidence for reducing gut permeability in clinical studies. However, probiotics work significantly more effectively when the dietary environment supports their establishment — meaning prebiotic fibre from diverse plant foods must be present. A probiotic supplement taken alongside a diet that continues to disrupt the gut microbiome is unlikely to produce significant sustained benefit. Food-first, supplements second.
Sources
- Cani, P.D. et al. (2007). Metabolic endotoxaemia initiates obesity and insulin resistance. Diabetes, 56(7).
- Chassaing, B. et al. (2015). Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature, 519.
- Guo, S. et al. (2013). Lipopolysaccharide regulation of intestinal tight junction permeability. American Journal of Physiology, 305(6).
- Wastyk, H.C. et al. (2021). Gut-microbiota-targeted diets modulate human immune status. Cell, 184(16).
- Leclercq, S. et al. (2014). Intestinal permeability, gut-bacterial dysbiosis, and behavioral markers of alcohol-dependence severity. PNAS, 111(42).
- Hollander, D. (1999). Intestinal permeability, leaky gut, and intestinal disorders. Current Gastroenterology Reports, 1(5).
- Carabotti, M. et al. (2015). The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Annals of Gastroenterology, 28(2).
- López-Moreno, A. et al. (2021). Dietary fat and gut microbiota interactions determine diet-induced obesity in mice. Nutrients, 13(4).
Related Articles
- The Gut-Hormone Connection: How Your Microbiome Shapes Menopause
- Perimenopause Bloating: Why You Feel 6 Months Pregnant After Every Meal
- Perimenopause Brain Fog: The Food-Brain Link No One Talks About
- Why Seed Oils Are Secretly Making Your Menopause Symptoms Worse