Phytoestrogens are one of the most discussed — and most misunderstood — topics in menopause nutrition. Depending on which source you read, they are either nature’s answer to HRT, dangerous hormone disruptors that cause cancer, or somewhere in the complicated middle ground where most nutritional science actually lives.
If you have spent any time in the perimenopause or menopause space, you have almost certainly encountered conflicting advice about soy. Eat it every day — it reduces hot flashes. Avoid it completely — it disrupts your thyroid. It causes breast cancer. It prevents breast cancer. The noise is significant, and most of it is not particularly useful to a woman trying to make a practical decision about what to eat for breakfast.
This article cuts through that noise. Not by dismissing the complexity or oversimplifying the evidence, but by looking honestly at what the peer-reviewed research actually shows — what phytoestrogens are, how they work, which ones have the strongest evidence for menopause symptom relief, and what the safety picture genuinely looks like for the foods most women are wondering about.
The answer is more nuanced than either camp suggests — and more practically useful.
Episode: “Phytoestrogens and Menopause — The Evidence Without the Agenda” — Real Food Science Podcast
Key Takeaways
- Phytoestrogens are plant compounds that weakly bind to oestrogen receptors — they are not oestrogen, and they do not behave identically to oestrogen in the body
- The three main classes — isoflavones, lignans, and coumestans — have different food sources, different potencies, and different evidence bases for menopause symptom relief
- The strongest evidence is for isoflavones from soy foods reducing hot flash frequency and severity — with a 2021 meta-analysis showing approximately 20% reduction in hot flash frequency
- Lignans from flaxseed have specific evidence for hot flash reduction and oestrogen metabolism support through the estrobolome
- The safety concerns around soy and breast cancer are largely based on animal studies — population-level data from Asian populations consuming soy throughout life does not support elevated risk
- Individual response varies significantly — equol producers (women who convert soy isoflavones to the more potent equol in the gut) see stronger benefits than non-producers
- Phytoestrogens from whole food sources are safe for most women and complement rather than replace the broader anti-inflammatory dietary approach
What Phytoestrogens Actually Are
Phytoestrogens are a diverse group of plant-derived compounds that have a chemical structure similar enough to oestrogen that they can bind to oestrogen receptors in human tissue — though with considerably weaker affinity than endogenous oestrogen. “Phyto” simply means plant — so phytoestrogen means plant oestrogen, though this name is somewhat misleading because they are not oestrogen and do not function identically to it.
There are three main classes relevant to menopause nutrition:
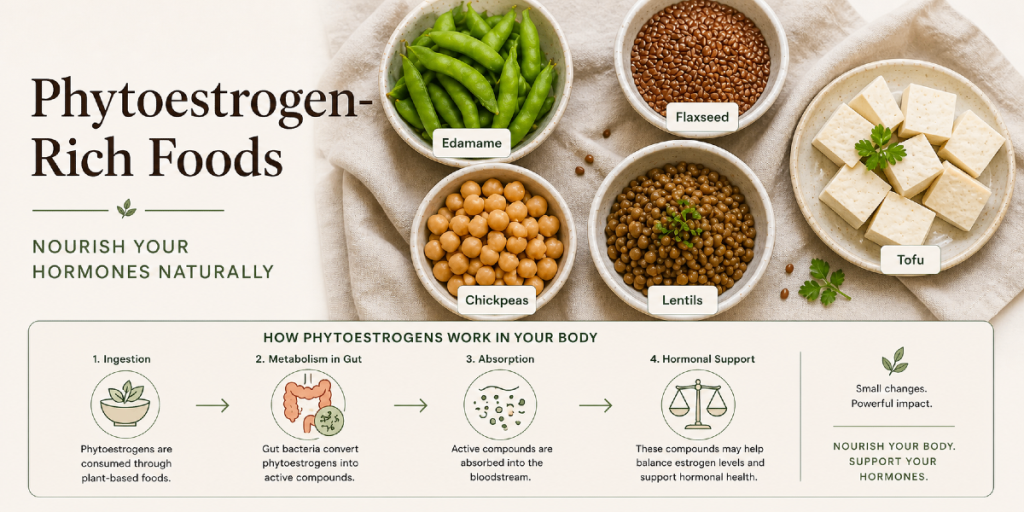
Isoflavones — found primarily in soy and soy products (edamame, tofu, tempeh, miso, soy milk). The main isoflavones are genistein, daidzein, and glycitein. These are the most extensively studied phytoestrogens in relation to menopause, with the largest body of clinical research.
Lignans — found in flaxseed (the richest source by a significant margin), sesame seeds, whole grains, legumes, and certain fruits and vegetables. The main lignans are secoisolariciresinol diglucoside (SDG) in flaxseed, which gut bacteria convert to the active forms enterodiol and enterolactone. Lignans are also relevant to oestrogen metabolism through the estrobolome — the gut bacterial community that regulates oestrogen recycling, covered in the gut-hormone connection article.
Coumestans — found in sprouted legumes, particularly clover and alfalfa sprouts. Less commonly consumed in typical Western diets and less extensively studied than isoflavones or lignans.
The potency of phytoestrogens relative to endogenous oestrogen is considerably lower — typically 0.001 to 0.1% of the activity of oestradiol at the oestrogen receptor, depending on the tissue and receptor subtype. This relative weakness is actually clinically relevant — it means they can weakly stimulate oestrogen-responsive pathways when oestrogen is low (as in menopause) while potentially moderating excessive oestrogen activity when levels are high (as in oestrogen dominance in early perimenopause).
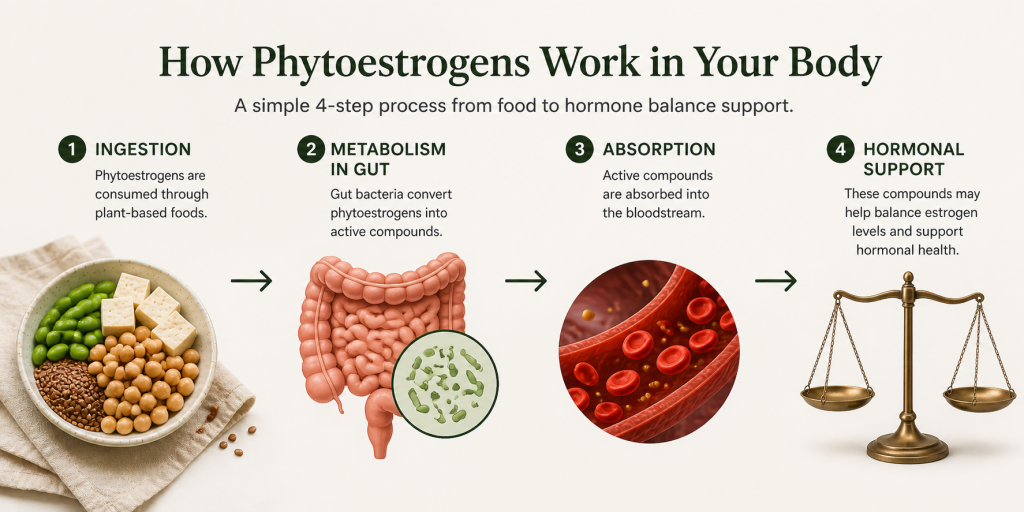
How Phytoestrogens Work in the Body — The Receptor Story
Understanding how phytoestrogens interact with oestrogen receptors explains why the evidence is more nuanced than simple “they work” or “they don’t work.”
There are two main oestrogen receptor subtypes in human tissue: oestrogen receptor alpha (ERα) and oestrogen receptor beta (ERβ). Endogenous oestrogen binds to both, producing effects in reproductive tissue, bone, cardiovascular tissue, brain, and gut. Phytoestrogens — particularly isoflavones — preferentially bind to ERβ, which is found in high concentrations in bone, brain, and cardiovascular tissue, but in lower concentrations in breast and uterine tissue than ERα.
This receptor selectivity has two important clinical implications:
First, it may explain why phytoestrogens produce measurable benefits in areas like bone protection, cardiovascular health, and cognitive function — where ERβ is highly expressed — while having less pronounced effects on reproductive tissue.
Second, it is the basis for the theoretical safety argument in relation to breast cancer risk — because breast tissue expresses proportionally more ERα than ERβ, phytoestrogens theoretically have less stimulatory effect on breast tissue than endogenous oestrogen.
The Evidence for Hot Flash Reduction
Hot flash frequency and severity is the most studied endpoint for phytoestrogen interventions, and the evidence is the strongest in this area.
Soy isoflavones
A 2021 meta-analysis published in Menopause — the journal of the Menopause Society — reviewed 17 randomised controlled trials and found that soy isoflavone supplementation reduced hot flash frequency by approximately 20% and severity by 26% compared to placebo. These effect sizes are modest compared to HRT but are clinically meaningful, particularly for women who cannot or choose not to use hormone therapy.
The dose used in most trials showing significant benefit was 40-80mg of total isoflavones daily — approximately the amount provided by one to two servings of soy food. Edamame provides approximately 18mg per 100g serving. A serving of firm tofu provides approximately 20-35mg. Tempeh provides approximately 40mg per 100g serving.
An important nuance: the isoflavone daidzein is converted in the gut by certain bacterial species into equol — a more potent oestrogenic compound than daidzein itself. Approximately 30-50% of Western women are equol producers — those who harbour the necessary gut bacteria. Equol producers consistently show stronger benefits from soy isoflavone interventions than non-producers. This is one reason the research shows such variable individual responses — roughly half of women will see stronger effects than the trial averages suggest, and half will see weaker effects.
Flaxseed lignans
A 2007 randomised trial published in the Journal of the Society for Integrative Oncology found that women eating approximately 40g of ground flaxseed daily for six weeks reported a 57% reduction in hot flash frequency and a 70% reduction in hot flash scores — results comparable to some hormone therapy trials in that study population.
Ground flaxseed is the richest dietary source of lignans — providing approximately 300mg of SDG per 100g, compared to the next richest sources (sesame seeds at approximately 29mg per 100g, sunflower seeds at approximately 11mg per 100g). The key is that the seeds must be ground — whole flaxseeds pass through the gut largely intact, with the lignans inside the seed coat inaccessible to gut bacteria.
Two tablespoons of ground flaxseed daily — approximately 14g — provides a meaningful lignan dose while also delivering ALA omega-3 and a useful fibre contribution. This is one of the most evidence-backed, low-cost, and practically simple additions available to perimenopausal women.
Red clover isoflavones
Red clover contains isoflavones including formononetin and biochanin A, which are converted in the gut to daidzein and genistein. Several trials using red clover supplements have shown modest reductions in hot flash frequency — the evidence is generally positive but less consistent than for soy isoflavones, partly because red clover products vary significantly in their isoflavone content.
The Evidence Beyond Hot Flashes
Bone density
Multiple clinical trials have found that soy isoflavones and flaxseed lignans have a modest protective effect on bone mineral density in postmenopausal women, likely through their preferential binding to ERβ in bone tissue. A 2010 meta-analysis in Osteoporosis International found that isoflavone supplementation was associated with significantly less bone mineral density loss in postmenopausal women compared to controls. The effect is smaller than HRT but meaningful as part of a comprehensive bone protection strategy alongside adequate calcium, vitamin D, and strength training.
Cardiovascular markers
The evidence for phytoestrogens and cardiovascular risk markers is reasonably consistent — soy protein and isoflavones are associated with modest reductions in LDL cholesterol and improvements in endothelial function in postmenopausal women. The American Heart Association’s position has evolved from endorsing soy protein for cardiovascular health to a more cautious view of the evidence, but the direction of effect remains positive in most trials.
Cognitive function
Several trials have examined isoflavones and cognitive function in postmenopausal women with mixed results. A 2012 study found that 25mg daily isoflavone supplementation improved measures of cognitive speed and memory in recently postmenopausal women. The cognitive benefits appear more consistent in women who are closer to menopause — suggesting a potential role in the cognitive transition period that aligns with the ERβ expression in hippocampal tissue.
Oestrogen metabolism and the estrobolome
Lignans from flaxseed interact with the estrobolome — the gut bacterial community covered in the gut-hormone connection article — in ways that may support healthier oestrogen metabolism and recycling. Women with higher lignan intake show different urinary oestrogen metabolite profiles, with proportionally higher levels of protective 2-hydroxyoestrone relative to more proliferative oestrogen metabolites. This oestrogen metabolite balance is increasingly recognised as clinically relevant to hormonal health.

The Safety Questions — Addressed Honestly
Phytoestrogens and breast cancer
This is the question most women ask first and most urgently. The short answer is that the population-level evidence does not support the concern — but the nuance matters.
The concern arose from animal studies in which very high doses of isolated isoflavones stimulated oestrogen-sensitive breast cancer cell growth in rodent models. These studies used doses far in excess of what any human diet would provide and involved forms of isoflavones that differ from those in whole food sources.
Human epidemiological data tells a different story. Multiple large-scale studies of Asian populations — who consume significant amounts of soy throughout life — show either no elevated breast cancer risk or reduced risk compared to low-soy populations. A 2014 meta-analysis in the American Journal of Clinical Nutrition found that higher soy intake was associated with a significant reduction in breast cancer risk in Asian women and no significant association in Western women.
The current position of most major cancer research organisations — including Cancer Research UK and the American Cancer Society — is that whole soy food consumption is safe for women with or without a history of breast cancer, based on the available evidence. This does not extend unequivocally to high-dose isolated isoflavone supplements taken over years — but it does apply to the food-first approach advocated throughout Real Food Science.
The nuanced honest answer: whole soy food consumption at two to three servings per week is not associated with increased breast cancer risk in the literature, and may be associated with modest reduction in risk. If you have a personal or family history of hormone-sensitive cancer, discuss with your oncologist before significantly increasing soy intake — not because the evidence mandates avoidance, but because the conversation belongs in that clinical relationship.
Phytoestrogens and thyroid function
Soy isoflavones have the potential to inhibit thyroid peroxidase — an enzyme involved in thyroid hormone production — at high doses. In women with adequate iodine status and no underlying thyroid dysfunction, this effect is not clinically significant at normal dietary intake levels. In women with hypothyroidism taking levothyroxine, large amounts of soy may interfere with medication absorption — the practical advice is to leave at least four hours between taking thyroid medication and consuming significant soy.
If you have a diagnosed thyroid condition, discuss soy intake with your prescribing clinician. If you have normal thyroid function, regular dietary soy is not a concern at food quantities.
Phytoestrogens and HRT
Phytoestrogens from whole food sources are safe to consume alongside HRT — the quantities delivered through food are far too small to meaningfully interact with prescribed hormone doses. Anti-inflammatory foods and HRT work in parallel rather than in competition. Many women find that the combination produces better symptom outcomes than either approach alone.
The Individual Response Question — Why Results Vary
If you have tried eating soy regularly and noticed no change in your hot flash frequency, it does not necessarily mean phytoestrogens are not for you. The most significant variable in phytoestrogen response is equol producer status — whether your gut bacteria can convert the soy isoflavone daidzein into equol.
Equol is significantly more potent than daidzein in binding to ERβ and producing oestrogenic effects. Equol producers — approximately 30-50% of Western women, compared to 50-70% of Asian women whose gut bacteria have been exposed to soy throughout life — see measurably stronger benefits from soy isoflavone interventions in clinical trials.
You cannot know your equol producer status without testing, but there are indirect indicators. If you have been eating soy regularly for several weeks without noticing any change in vasomotor symptoms, you may be a non-producer — in which case lignans from flaxseed, which do not rely on equol conversion, may produce stronger effects for you.
Gut microbiome diversity also influences lignan conversion — enterolignans are produced by gut bacteria, so a depleted microbiome reduces the conversion rate. This is one more reason why the gut health interventions covered in the 30 plants article and the gut-hormone connection article are relevant to phytoestrogen efficacy — building microbiome diversity improves the conversion of both soy isoflavones to equol and flaxseed lignans to active enterolignans.
The Practical Phytoestrogen Strategy
Based on the evidence, here is the practical approach for women in perimenopause and menopause:
Start with ground flaxseed daily Two tablespoons daily — in porridge, yoghurt, smoothies, or salad dressings. This is the highest-lignan food available, the evidence for hot flash reduction is strong, and it delivers ALA omega-3 and fibre simultaneously. Grind whole seeds yourself (coffee grinder) or buy pre-ground and store in the fridge. Cost: approximately £2-3 per month.
Add one to two servings of whole soy food per day Edamame as a snack, tofu in stir-fries, tempeh in salads, miso in soups. Aim for 40-80mg of isoflavones daily — achievable through one to two servings of soy food. If you have never eaten soy regularly, introduce it gradually over two to three weeks while monitoring symptoms.
Include legumes broadly Chickpeas, lentils, black beans — all provide modest amounts of isoflavones and contribute to the plant diversity that supports equol production. These are cornerstone anti-inflammatory foods independently of their phytoestrogen content.
Track your symptoms Because individual response to phytoestrogens varies significantly — particularly between equol producers and non-producers — systematic symptom tracking is more useful here than for almost any other dietary intervention. The Menopause Symptom Tracker linked below gives you the structure to track hot flash frequency, severity, and other symptom measures consistently so you can see whether the dietary change is producing the expected benefit within your specific biology.
Give it eight to twelve weeks The evidence suggests that meaningful reductions in hot flash frequency from phytoestrogen interventions emerge over six to twelve weeks of consistent intake. Less than four weeks is insufficient to draw conclusions about your individual response.
Free Resource: Start Tracking Before You Start Changing
Symptom tracking before and during any dietary intervention is what converts vague impressions into actionable data. Without a baseline, you cannot see whether the change is working.
→ Download the free Menopause Bloat Trigger Checklist — identify your personal bloating and inflammation pattern before adding new foods, so you can distinguish phytoestrogen benefits from other dietary effects.
Go Deeper: The Menopause Symptom Tracker
The Menopause Symptom Tracker gives you a structured daily log covering all twelve core menopause symptoms — including hot flash frequency and severity, sleep quality, mood, and digestive symptoms — with a monthly pattern view that makes individual food and lifestyle correlations visible over time. Essential for any woman testing phytoestrogen foods and wanting to know whether they are working.
FAQ
How much soy is too much? The evidence suggests that two to three servings of whole soy food daily is well within a safe and beneficial range for most women. The concerns about soy relate primarily to isolated isoflavone supplements at very high doses over extended periods — not to whole soy food consumption. Two servings of edamame or tofu per day provides approximately 40-70mg of isoflavones — within the range showing clinical benefit without approaching the doses used in studies raising theoretical concerns.
Can I get enough phytoestrogens from flaxseed alone without eating soy? Yes. Flaxseed lignans and soy isoflavones work through overlapping but not identical mechanisms. Women who choose not to eat soy — for taste, ethical, or medical reasons — can meaningfully support phytoestrogen intake through two tablespoons of ground flaxseed daily, legumes broadly, sesame seeds, and wholegrains. The evidence for flaxseed specifically is strong enough to stand alone as a phytoestrogen strategy.
I am on tamoxifen — can I eat phytoestrogen foods? This is a clinical question that requires discussion with your oncologist. The theoretical concern is that phytoestrogens could compete with tamoxifen at the oestrogen receptor. Current guidance varies — some oncologists advise caution with soy foods during tamoxifen treatment, others do not. Do not make this decision based on a nutrition article — have the conversation with your prescribing clinician who knows your specific situation.
Do phytoestrogens help with symptoms other than hot flashes? Yes — as covered above, the evidence extends to modest bone protection, cardiovascular marker improvement, and potentially cognitive function. Lignan metabolism through the estrobolome also supports healthier oestrogen metabolite profiles. The evidence outside of hot flashes is less consistent and the effect sizes are smaller, but the direction is positive across multiple relevant endpoints.
Will eating phytoestrogens affect my HRT dose? No — the amounts of phytoestrogens from whole food sources are far too small to meaningfully interact with prescribed HRT doses. They do not substitute for HRT or alter its pharmacological action. They are complementary dietary elements, not competing interventions.
Sources
- Messina, M. (2016). Soy and health update: evaluation of the clinical and epidemiologic literature. Nutrients, 8(12).
- Franco, O.H. et al. (2016). Use of plant-based therapies and menopausal symptoms: a systematic review and meta-analysis. JAMA, 315(23).
- Pruthi, S. et al. (2007). Pilot evaluation of flaxseed for the management of hot flashes. Journal of the Society for Integrative Oncology, 5(3).
- Morabito, N. et al. (2002). Effects of genistein and hormone-replacement therapy on bone loss in early postmenopausal women. Journal of Bone and Mineral Research, 17(10).
- Shu, X.O. et al. (2009). Soy food intake and breast cancer survival. JAMA, 302(22).
- Atkinson, C. et al. (2004). The effects of phytoestrogen isoflavones on bone density in women. American Journal of Clinical Nutrition, 79(2).
- Guha, N. et al. (2009). Soy isoflavones and risk of cancer recurrence in a cohort of breast cancer survivors. Breast Cancer Research and Treatment, 118(2).
Related Articles
- 7 Foods That Help Hot Flashes Naturally
- The Gut-Hormone Connection: How Your Microbiome Shapes Menopause
- 30 Plants a Week: The Gut Diversity Goal That Could Transform Your Menopause
- Perimenopause Bloating: Why You Feel 6 Months Pregnant After Every Meal