
If there is one nutritional shift that explains more about the chronic inflammation epidemic — and the worsening of menopause symptoms in women eating modern Western diets — than almost any other, it is this: the collapse of the omega-6 to omega-3 ratio.
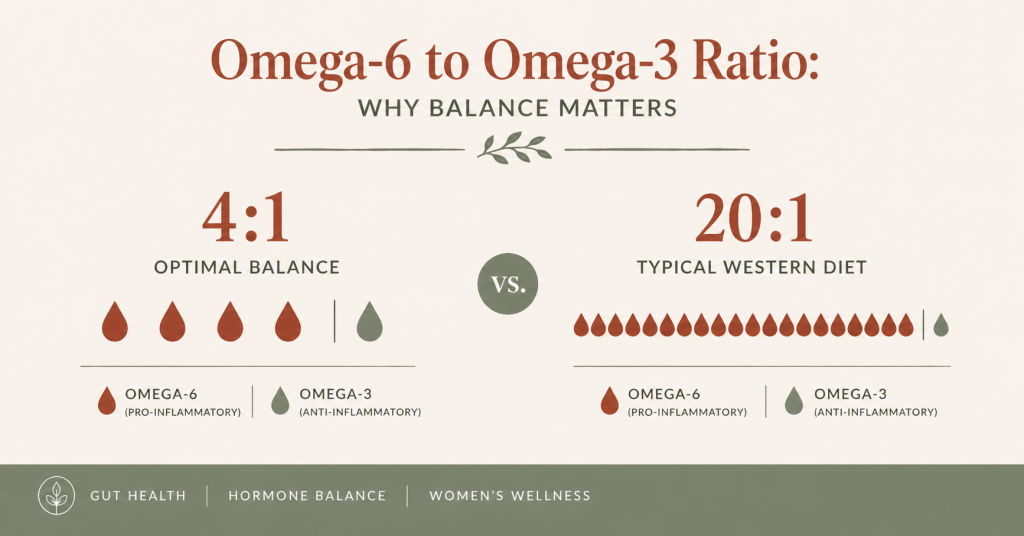
For most of human evolutionary history, people consumed omega-6 and omega-3 fatty acids in roughly equal amounts — a ratio of approximately 1:1 to 4:1. Today, the average Western diet delivers a ratio somewhere between 15:1 and 20:1 in favour of omega-6. That shift — driven almost entirely by the industrialisation of seed oils and the displacement of traditional whole food fats — has happened within the last 100 years. Our inflammatory biology has not caught up.
For women in perimenopause and menopause, where the protective anti-inflammatory buffer of oestrogen is already withdrawing, this omega-6 overload does not merely contribute to background inflammation. It amplifies the hormonal transition itself — worsening hot flashes, intensifying joint pain, deepening brain fog, disrupting sleep, and accelerating the gut permeability changes that drive a cascade of further symptoms.
Understanding the omega-6 to omega-3 ratio is not advanced nutritional biochemistry. It is one of the most practical and immediately actionable areas of nutrition science available to women in midlife — because shifting the ratio is largely a matter of swapping a handful of everyday foods.
[Podcast Player Block — Episode: “The Omega-6 Overload — Why the Modern Diet Is Making Menopause Worse” — Real Food Science Podcast]
Key Takeaways
- The omega-6 to omega-3 ratio in the modern Western diet sits at approximately 15-20:1 — far above the 1:1 to 4:1 ratio at which human inflammatory biology evolved
- Omega-6 and omega-3 compete for the same enzymes — when omega-6 dominates, the balance of inflammatory versus anti-inflammatory signalling molecules shifts decisively toward inflammation
- For women in perimenopause and menopause, where oestrogen’s anti-inflammatory protection is declining, the omega-6 overload amplifies every inflammation-driven symptom
- The primary driver of omega-6 overload is seed oil consumption — in cooking oils and throughout packaged foods
- Shifting the ratio requires both reducing omega-6 intake and increasing omega-3 intake — the two levers work together
- Measurable changes in the omega-6 to omega-3 ratio in cell membranes occur within four to eight weeks of sustained dietary change
What Omega-6 and Omega-3 Fatty Acids Actually Are
Before getting into the ratio and its consequences, it helps to understand what these fatty acids actually are and why the body needs both.
Omega-6 and omega-3 are polyunsaturated fatty acids — fats with multiple double bonds in their carbon chain. They are classified as essential fatty acids because the human body cannot synthesise them and must obtain them from food. Both are required for normal biological function. Neither is inherently bad.
The primary dietary omega-6 fatty acid is linoleic acid (LA) — found in high concentrations in seed oils (sunflower, corn, soybean, rapeseed), nuts, and to a lesser extent in animal products. The body converts linoleic acid into longer-chain omega-6 fatty acids, most significantly arachidonic acid (AA).
The primary dietary omega-3 fatty acids are alpha-linolenic acid (ALA) — found in flaxseed, walnuts, and chia seeds — and the long-chain EPA and DHA found in oily fish and algae. The body can convert ALA to EPA and DHA, but this conversion is inefficient — typically only 5-10% — which is why direct dietary sources of EPA and DHA from oily fish are so important.
The critical point is what each fatty acid is converted into. Arachidonic acid — the downstream omega-6 product — is the precursor for a family of pro-inflammatory signalling molecules called eicosanoids: prostaglandins, thromboxanes, and leukotrienes that drive inflammation, pain signalling, blood clotting, and immune activation. EPA and DHA — the downstream omega-3 products — are converted into a different family of eicosanoids that are anti-inflammatory, vasodilatory, and pro-resolving.
Both families are necessary. The balance between them determines your inflammatory tone.
The Enzyme Competition — Why the Ratio Matters More Than Absolute Amounts
The reason the ratio between omega-6 and omega-3 matters so much is the enzyme competition that sits at the centre of both pathways.
The enzymes that convert linoleic acid to arachidonic acid — delta-6-desaturase and delta-5-desaturase — are the same enzymes that convert ALA to EPA and DHA. When omega-6 massively dominates the diet, these enzymes are almost entirely occupied processing linoleic acid. Very little capacity remains for omega-3 conversion.
The consequences are twofold. First, arachidonic acid accumulates — providing more raw material for pro-inflammatory eicosanoid production. Second, EPA and DHA production is suppressed — reducing the availability of anti-inflammatory and pro-resolving mediators. The inflammatory balance tips in both directions simultaneously.
At a ratio of 4:1 or lower, these enzyme systems process both pathways adequately — producing a balanced inflammatory signalling environment. At the modern ratio of 15-20:1, the omega-3 pathway is effectively outcompeted. The result is a chronic pro-inflammatory state that is not driven by any acute immune challenge — it is simply the baseline of the modern dietary pattern.
How the Omega-6 Overload Specifically Affects Menopause
The omega-6 to omega-3 ratio influences inflammation throughout the body and across the lifespan. But for women in perimenopause and menopause, the effect is amplified through a specific interaction with declining oestrogen.
Oestrogen has direct anti-inflammatory properties — it suppresses certain inflammatory cytokines, moderates immune cell activity, and reduces the conversion of arachidonic acid to pro-inflammatory prostaglandins. While oestrogen levels are adequate, the inflammatory consequences of a high omega-6 diet are partly buffered by this hormonal protection.
As oestrogen declines during perimenopause, that buffering diminishes. The same omega-6 load that was producing manageable background inflammation at 38 now produces a more pronounced and more symptomatic response at 46. Women notice that symptoms they had barely registered — occasional joint stiffness, mild bloating after certain meals, a slightly slower cognitive recovery after poor sleep — suddenly become persistent, disabling, and disproportionate to any obvious cause.
The omega-6 overload has not changed. The body’s ability to buffer it has.
Specific menopause symptoms directly driven by the omega-6 to omega-3 imbalance include:
Hot flashes. Prostaglandins derived from arachidonic acid — the downstream omega-6 product — directly modulate the hypothalamic thermostat. Elevated AA-derived prostaglandins narrow the thermoneutral zone, increasing the frequency of vasomotor responses. Multiple studies have found that women with higher blood omega-3 levels report fewer and less severe hot flashes compared to those with higher omega-6 levels.
Joint pain and stiffness. Arachidonic acid is the direct substrate for the COX-2 enzyme — the enzyme that produces the inflammatory prostaglandins driving joint inflammation. This is the same pathway targeted by NSAIDs like ibuprofen. A diet chronically high in omega-6 provides the raw material for this pathway continuously. Shifting the ratio toward omega-3 reduces the substrate available for COX-2 and provides EPA and DHA as competitive inhibitors of the pathway itself.
Brain fog and mood. DHA is a structural component of neuronal cell membranes — it makes up approximately 30-40% of the polyunsaturated fatty acids in the brain. When the omega-6 to omega-3 ratio is high, omega-6 fatty acids displace DHA from neuronal membranes, reducing membrane fluidity and impairing synaptic transmission. Reduced DHA availability correlates with worse cognitive performance, lower mood, and increased neuroinflammation — all contributors to the cognitive symptoms of perimenopause.
Gut permeability. As covered in the leaky gut article, high omega-6 polyunsaturated fats — particularly their oxidation products produced under heat — directly disrupt tight junction proteins in the gut lining. EPA and DHA, conversely, support tight junction integrity and reduce the LPS-driven inflammatory signalling that follows gut permeability.
Sleep quality. EPA and DHA influence the production of serotonin and melatonin through their effects on the tryptophan conversion pathway. Women with higher omega-3 status consistently show better sleep quality measures — earlier sleep onset, more restorative sleep, fewer wakings. The 2-3am waking pattern driven partly by nocturnal cortisol spikes is also moderated by omega-3’s direct cortisol-blunting effect at the pituitary level.
The Two Levers — Reducing Omega-6 and Increasing Omega-3
Shifting the omega-6 to omega-3 ratio requires working both levers simultaneously. Reducing omega-6 alone without increasing omega-3 improves the ratio but does not maximise the anti-inflammatory benefit. Increasing omega-3 without reducing omega-6 is partially effective but remains limited by enzyme competition.
Lever 1: Reducing omega-6
The primary omega-6 source in the modern diet is seed oils — used in everyday cooking and present throughout packaged foods. As covered in detail in the seed oils article and the hidden seed oils article, replacing seed oil cooking fats with olive oil, butter, and ghee produces the most significant single reduction in daily omega-6 intake available through dietary change.
Packaged food audit comes second — most processed foods contain seed oils as a primary ingredient. Removing the highest-omega-6 packaged foods from your regular purchasing (granola made with seed oils, shop-bought hummus, flavoured crackers, processed dressings) makes a meaningful additional reduction.
A typical woman eating a standard Western diet consumes approximately 20-30g of linoleic acid daily. Replacing cooking oils and eliminating the highest-omega-6 packaged foods can reduce this to 8-12g daily — approximately the level at which the ratio begins to approach a more physiologically appropriate range, assuming adequate omega-3 intake.
Lever 2: Increasing omega-3
The omega-3 target for meaningful anti-inflammatory effect in perimenopausal women is:
- EPA and DHA combined: 2-3g daily — achievable through two to three portions of oily fish per week plus supplementation if needed
- ALA: approximately 2g daily from plant sources as an additional contribution (walnuts, ground flaxseed, chia seeds)
Oily fish is the highest-priority omega-3 source because it provides EPA and DHA directly — the biologically active forms that do not require the inefficient ALA conversion step. Salmon, mackerel, sardines, anchovies, and trout are the richest sources. Tinned sardines and mackerel are affordable, sustainable, and nutritionally equivalent to fresh.
For women who do not eat oily fish, algae-based omega-3 supplements are the only direct plant-based source of EPA and DHA. These are produced from the same algae that fish consume — making them nutritionally equivalent without the fishy aftertaste.
Ground flaxseed, walnuts, and chia seeds provide ALA — which converts to EPA at approximately 5-10% efficiency and to DHA at lower rates still. While these are valuable additions that contribute to overall omega-3 status, they should not be the sole omega-3 strategy for women seeking meaningful inflammatory benefit.

Where Spices and Herbs Fit In
Reducing omega-6 and increasing omega-3 addresses the fatty acid ratio directly. But there is a parallel dietary lever that works on the same inflammatory pathways through different mechanisms: the polyphenols and bioactive compounds in anti-inflammatory spices and herbs.
Turmeric’s curcumin, ginger’s gingerol, rosemary’s rosmarinic acid, and the flavonoids in oregano and thyme all inhibit NF-κB — the master transcription factor of inflammatory gene expression — through mechanisms that overlap with and complement the omega-3 pathway. These compounds do not correct the fatty acid ratio, but they reduce the inflammatory signalling downstream of arachidonic acid regardless of the ratio — making them particularly valuable as a complementary strategy.
For women working to shift their omega-6 to omega-3 balance, adding therapeutic amounts of anti-inflammatory spices to daily cooking provides an additional anti-inflammatory mechanism that compounds with the fatty acid rebalancing. The evidence behind the top ten anti-inflammatory spices and herbs — including specific effective amounts and the mechanisms behind each one — is covered in full in the Top 10 Anti-Inflammatory Spices & Herbs guide linked below.
The Timeline — What to Expect as the Ratio Shifts
The omega-6 to omega-3 ratio in cell membranes changes gradually rather than immediately — because membrane remodelling requires existing fatty acids to be replaced during normal cell turnover. Different tissues turn over at different rates:
Red blood cells: 120-day lifespan — measurable changes in red blood cell fatty acid composition (the most reliable biomarker of dietary omega-3 status) occur over four to eight weeks of consistent dietary change.
Neuronal membranes: Longer-lived — significant cognitive benefits from omega-3 rebalancing typically emerge over eight to sixteen weeks of consistent intake.
Inflammatory signalling: More immediate — the reduction in arachidonic acid substrate for prostaglandin production begins within days of reducing omega-6 intake. Acute inflammatory markers can shift within two to four weeks.
The practical implication is that the ratio shift is a sustained intervention rather than a quick fix — but one where most women begin noticing symptomatic improvements within two to four weeks, with deeper benefits continuing to accumulate over two to three months of consistent dietary change.
Practical Weekly Omega-3 Target
Here is a concrete weekly food plan that achieves the omega-3 target while contributing to omega-6 reduction simultaneously:
Monday: Tinned sardines on rye toast with olive oil for lunch Tuesday: Salmon fillet for dinner — 100g provides approximately 2g EPA+DHA Wednesday: Ground flaxseed (2 tbsp) in morning porridge or yoghurt — approximately 3.2g ALA Thursday: Mackerel fillet for dinner — approximately 2.5g EPA+DHA Friday: Walnut handful with afternoon snack — approximately 2.5g ALA Saturday: Smoked salmon with eggs for breakfast Sunday: Sardine or tuna salad for lunch — or a second salmon dinner
That weekly pattern delivers approximately 10-12g combined EPA and DHA across the week — well above the anti-inflammatory threshold — alongside a meaningful ALA contribution from plant sources. Combined with the cooking oil swap covered in the cooking fats article, this approaches the dietary pattern that research consistently associates with lower inflammatory markers and reduced menopause symptom severity.
Free Resource: Identify Your Inflammation Triggers
Before building out a full omega-3 strategy, understanding your personal inflammatory pattern helps you identify which symptoms are most directly driven by fatty acid imbalance versus other contributors.
→ Download the free Menopause Bloat Trigger Checklist — a five-minute checklist that identifies your personal inflammation and bloating triggers, including several directly linked to the omega-6 to omega-3 imbalance.
Go Deeper: Top 10 Anti-Inflammatory Spices & Herbs
The Top 10 Anti-Inflammatory Spices & Herbs guide covers the ten spices and herbs with the strongest evidence for reducing inflammatory signalling in perimenopausal and menopausal women — including the specific compounds, effective amounts, and how to incorporate each one into everyday cooking to complement your omega-3 strategy.
FAQ
Do I need to take fish oil supplements or can I get enough omega-3 from food alone? Two to three portions of oily fish per week provides approximately the same EPA and DHA as a daily 1-2g fish oil supplement. For women who eat oily fish regularly, food sources are sufficient. For those who eat oily fish rarely or not at all, a high-quality fish oil or algae-based supplement providing at least 1g combined EPA and DHA daily is a practical addition. Look for supplements with a third-party purity certification — omega-3 supplements vary significantly in quality and oxidation levels.
Is the omega-6 to omega-3 ratio the same concern for vegetarians and vegans? Yes — and potentially more so, because plant-based diets often include significant amounts of omega-6 from nuts, seeds, and plant oils while relying on ALA for omega-3, which converts inefficiently. Vegetarians and vegans should prioritise algae-based EPA and DHA supplements, minimise seed oil cooking fats, and maximise ALA sources (ground flaxseed, chia seeds, walnuts, hemp seeds). The ratio concern is diet-pattern independent — it is the absolute balance that matters, not whether the foods are animal or plant based.
What is the omega-6 content of olive oil — does it contribute to the overload? Extra virgin olive oil is approximately 73% monounsaturated oleic acid (omega-9) and approximately 10-11% linoleic acid (omega-6). While olive oil does contain omega-6, its content is significantly lower than seed oils (sunflower oil is 65% linoleic acid), and the oleic acid does not compete in the same enzyme pathways as omega-6. Olive oil does not meaningfully contribute to omega-6 overload when used as the primary cooking fat — which is why it is the recommended replacement in the cooking fat swap.
How do I know if my omega-6 to omega-3 ratio is improving? The most accurate measure is an omega-3 index blood test — which measures EPA and DHA as a percentage of total red blood cell fatty acids. This test is available through several private health testing services and provides a baseline and progress measure. However, most women find that symptomatic improvement — reduced joint stiffness, improved sleep quality, better cognitive clarity — is a reliable proxy indicator that the ratio is shifting in the right direction, even without testing.
Is there a point where omega-3 can be too high? Very high omega-3 intake — above 5g EPA and DHA daily from supplements — can have blood-thinning effects relevant to women on anticoagulant medications. At dietary levels from food (two to three portions of oily fish per week) and standard supplement doses (1-3g daily), there are no clinically significant adverse effects in otherwise healthy women. Discuss with your GP if you are taking blood-thinning medications.
Sources
- Simopoulos, A.P. (2016). An increase in the omega-6/omega-3 fatty acid ratio increases the risk for obesity. Nutrients, 8(3), 128.
- Calder, P.C. (2017). Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochemical Society Transactions, 45(5).
- Lucas, M. et al. (2009). Ethyl-eicosapentaenoic acid for the treatment of psychological distress and depressive symptoms in middle-aged women. Menopause, 16(2).
- Yehuda, S. et al. (2005). The role of polyunsaturated fatty acids in restoring the aging neuronal membrane. Neurochemical Research, 30(6-7).
- Ramsden, C.E. et al. (2013). Use of dietary linoleic acid for secondary prevention of coronary heart disease. British Medical Journal, 346.
- Blasbalg, T.L. et al. (2011). Changes in consumption of omega-3 and omega-6 fatty acids in the United States during the 20th century. American Journal of Clinical Nutrition, 93(5).
- Peet, M. & Stokes, C. (2005). Omega-3 fatty acids in the treatment of psychiatric disorders. Drugs, 65(8).